

Every Other State Has Built a Secure Facility for Defendants Found Mentally Incompetent to Stand Trial. Have Vermont Lawmakers Even Looked at How They Did It?
While many states have found a model that fairly meets major concerns, a different faction blocks whatever Vermont proposes. The result: five years of debate, zero facilities, and people are dead.

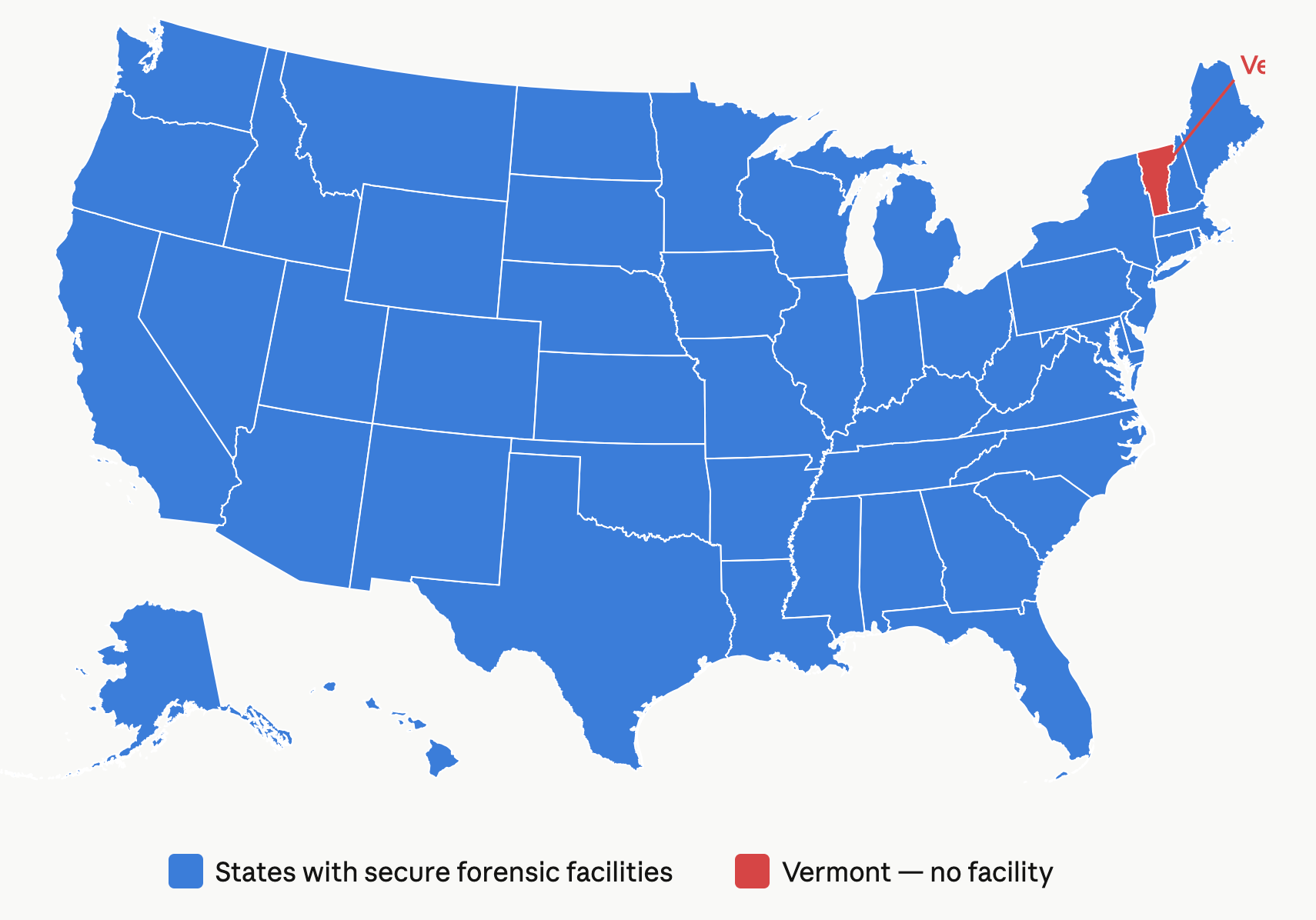
If someone in your town is charged with murder and found mentally incompetent to stand trial, what happens next depends on where you live. In most states, there is a secure treatment facility designed for that situation — a place where the defendant receives competency restoration services in a locked clinical setting with periodic court review.
In Vermont, that place does not exist.
According to Karen Barber, General Counsel of the Department of Mental Health, Vermont may be the only state in the country without one.
S.193, the bill that would create one, passed the Vermont Senate 29–1 on April 1. As Compass Vermont has reported, three House committees have held hearings. None has voted. The session adjourns May 8.
The stated holdup is a policy disagreement: should the facility be run by the Department of Corrections, as the bill proposes, or by a health-oriented agency?
That sounds like a serious question. But the record shows that Vermont has now tried both approaches — and blocked both.
Vermont has tried this before. Every version failed.
In 2021, Act 57 created a working group to study the issue and recommend a path forward. By 2022, the group had fallen apart. DMH General Counsel Karen Barber told lawmakers the group “will likely not be able to put forward consensus recommendations.” Representative Alice Emmons, chair of House Corrections and Institutions, responded: “I find that very, very frustrating. For legislators, it puts us in a bind because we want to do what is the best for everyone, and we need direction from those folks who are involved in the system, and we’re not getting it.”
In 2023, the legislature authorized a nine-bed forensic unit at the Vermont Psychiatric Care Hospital in Berlin — a DMH-led model. It was never built.
In 2024, the House considered using empty beds at the River Valley Therapeutic Residence, a locked step-down facility under DMH. Instead, the House Human Services Committee stripped the facility entirely and replaced it with involuntary medication authority at Essex. No victims testified. According to Kelly Carroll, founder of the grassroots advocacy group Voices for Vermont Victims, Representative Theresa Wood stated during testimony that victim input was irrelevant because “all you bring is emotion.” Compass Vermont has not been able to verify this statement from the hearing record.
In 2026, S.193 flipped the model. Instead of DMH leading, the bill places the facility under DOC with clinical services layered in. Now the same lawmakers who could not advance the DMH model are objecting to the DOC model.
Meanwhile, Vermont did launch one program that works: FACT — Forensic Assertive Community Treatment — a collaboration between DOC, DMH, and Pathways Vermont that provides community-based support for justice-involved people with mental health challenges. It’s a multi-agency hybrid. It’s staffed. But it’s designed for lower-risk individuals, not defendants charged with murder who are found incompetent to stand trial. FACT is the front end. S.193 is the back end. They’re not in conflict — they’re meant to work together.
The result of five years: Vermont has explored DMH-led models, DOC-led models, community-based programs, and working groups. Each time, a different faction blocks whatever is proposed. The facility has never been built. The gap remains.
How other states answered the same question
National surveys by the National Research Institute show that most states use one or more of four approaches. Many use several.
Secure forensic hospitals run by mental health agencies. This is the most common model. California runs its Department of State Hospitals as a standalone agency. Washington State runs forensic services through two state hospitals under the Department of Social and Health Services. These are clinical facilities with security — not prisons with therapy rooms.
Forensic units inside existing psychiatric hospitals. The majority of state mental health agencies operate dedicated forensic units within their existing hospitals. For Vermont — where the projected caseload is approximately six admissions per year, according to testimony before the House — this would mean a secure wing inside an existing facility, staffed by clinicians, under DMH oversight.
Jail-based competency restoration. Texas, Georgia, Virginia, and California deliver restoration services inside county jails with clinical staff brought in. A seven-year study published in Criminal Justice and Behavior found these programs restored competency in 56 percent of patients over an average of 49 days. A Virginia pilot achieved 83 percent. These programs were developed to address the exact problem Vermont faces: forensic beds filling up, defendants stuck in jail without treatment.
Multi-agency hybrid models. In Fulton County, Georgia, a partnership between Emory University, the state Department of Behavioral Health, and the county jail created a continuum — outpatient, jail-based, dedicated unit, or full hospitalization — matched to each defendant’s clinical needs. About a third of defendants are diverted out of corrections entirely. In Miami-Dade County, the Forensic Alternative Center operates through Jackson Behavioral Health Hospital, a local nonprofit, and the court system’s Criminal Mental Health Project. Neither program is run by corrections or mental health alone. Both rejected the binary.
Vermont doesn’t have to invent a model. It has to pick one.
What happened in the one state that chose the DOC model
Bridgewater State Hospital in Massachusetts is widely cited as the only major forensic psychiatric facility in the country run by a corrections department rather than a mental health agency. It sits across the border from Vermont — and it is a cautionary tale.
In March 2026, the Boston Globe reported on a February 2025 review by Massachusetts’s Disability Law Center that found persistent problems at Bridgewater. The same for-profit contractor Vermont’s DOC uses — Wellpath — was providing clinical care. In 2020, the U.S. Department of Justice’s Civil Rights Division found patients in mental health crisis were placed “at serious risk of harm.” The facility has faced legal action over its use of restraints and seclusion. The DLC found no sign DOC was conducting meaningful oversight.
Wellpath, owned by the private equity firm H.I.G. Capital, declared bankruptcy in November 2024 with $644 million in debt and more than 1,500 lawsuits nationally.
Massachusetts Senator Cynthia Stone Creem is now sponsoring a bill to transfer Bridgewater to DMH. “If you’re the only state in the nation that allows a correctional agency to handle this, rather than the Department of Mental Health, that’s a problem,” Creem told the Globe.
If Vermont passes S.193 as written — with the facility under DOC — critics say it would move Vermont toward the Bridgewater model. Some Massachusetts lawmakers are seeking to move Bridgewater away from that model entirely.
Senator Tanya Vyhovsky, the lone no vote on S.193, has raised exactly these concerns. “When we’re talking about treatment best practices, those don’t happen in prisons,” she said during committee deliberations. Her objection is tied to documented concerns about correctional control and contractor performance.
But here is the question her position — and the position of every lawmaker who has opposed the bill in its current form — does not answer: if not DOC, then what? They tried DMH. It was blocked. They tried a working group. It collapsed. They tried a step-down facility. It was stripped. If not this, then what — and when?
Vermont finds the money — when it wants to
Vermont has demonstrated it can act fast on public health emergencies when it chooses to. Since 2022, the state has received more than $41 million in opioid settlement funds. According to the Vermont Attorney General’s office, approximately $23.9 million has been allocated for opioid crisis remediation since 2024. The legislature committed $5.3 million annually to syringe exchange programs, recovery housing, outreach, and a Burlington overdose prevention center. The legislature appropriated $6.2 million in FY 2024 for opioid treatment initiatives.
These are defensible investments. The opioid crisis has killed more than 1,500 Vermonters in the past decade.
But no capital appropriation for a forensic facility appears in any Vermont budget enacted during the five years this issue has been under legislative debate. During that period, supporters have cited the deaths of Emily Hamann, Karina Rheaume, and Hailey Colyer as evidence of dangerous gaps in the current system. A young woman was stabbed to death inside a state-arranged group home in Colchester while her caregiver was in the residence.
The legislature has not yet appropriated funds for a facility serving a population that testimony estimates at approximately six people per year.
This is not an argument against opioid spending. It is an observation about what the legislature treats as urgent and what it allows to wait.
The bottom line
The “DOC vs. DMH” debate is real. The concerns about Wellpath are documented. The constitutional questions are legitimate.
But this debate has now consumed five years, four bills, dozens of committee hearings, and one working group that couldn’t agree on anything — while most other states built systems using a variety of models. Many of those systems face their own capacity challenges. But they exist. Vermont is still debating whether to build one.
Jack McCullough of Vermont Legal Aid told the House Judiciary Committee in 2023 that the forensic facility bill was “a solution in search of a problem.” In April 2026, he offered a substantially similar assessment before the same committee. Three years apart, the same witness made the same argument. During that period, Karina Rheaume and Hailey Colyer were killed in cases cited by facility supporters as evidence of the gap.
Kelly Carroll — the Bennington mother whose daughter Emily Hamann was murdered in 2021 by a man who had been found incompetent, released into his mother’s custody without formal state supervision — wrote to the House committees on April 1: “We cannot continue to cycle through the same outcomes and expect different results.”
S.193 may not be the right bill. But the right response to the wrong bill is a better bill — not another five years of hearings.
Compass Vermont is free, independent, and has no ads, no sponsors, and no corporate owner. If you value reporting that gives you the full picture and lets you draw your own conclusions, please consider subscribing or upgrading to a paid subscription. Every subscription — free or paid — helps us keep doing this work.